What is Bladder Cancer?
Bladder cancer is a common malignancy in Australian society. This section aims to answer some frequently asked questions that arise when bladder cancer is diagnosed or suspected.
In 2015, 2747 new cases of bladder cancer were diagnosed in Australia. Bladder cancer is common in people over 60, and is significantly more common in men than in women.
At Katelaris Urology, we provide a comprehensive range of bladder cancer treatments appropriate to the grade and stage. We are one of the best and most experiences bladder cancer specialist in Sydney. The patient is carefully supported through the process with each treatment option carefully explained and discussed.
On this information page you can learn about the following:
- Causes of bladder cancer
- Bladder cancer staging and grading
- Bladder cancer symptoms
- Diagnosis of bladder cancer
- Bladder cancer treatment
- Treatment of superficial bladder cancer
- Treatment for carcinoma in situ
- Treatment for muscle-invasive bladder cancer
- Frequently asked questions
- Statistics
Bladder cancer causes
- Lifestyle: Smoking is the single greatest risk factor for bladder cancer; smokers have twice the risk of developing bladder cancer than non-smokers. There is also some evidence that diets that include a large number of fried meats and animal fats are associated with an increased risk of bladder cancer.
- Occupational exposure to industrial carcinogens: Chemicals that have been proven to increase the risk of developing cancer may also contribute, particularly exposure to aniline dyes. Workers in the rubber, leather, textile, hair colouring, paint and printing industries are at increased risk unless proper safety precautions are taken in the workplace.
- Treatment for other cancers: Cyclophosphamide (Cytoxan) is a chemotherapeutic agent that increases the risk of bladder cancer. Patients receiving Cytoxan should be monitored with at least urinary cytology on a regular basis. Pelvic radiation therapy (eg. for prostate cancer) also carries an increased risk of developing bladder cancer over a 5 – 15 year period.
Bladder cancer staging and grading
Bladder cancers are staged by how far they have invaded into the bladder wall. The bladder wall consists of three main layers: the mucosa (innermost layer), the submucosa, and the underlying muscular wall (outer most layer)
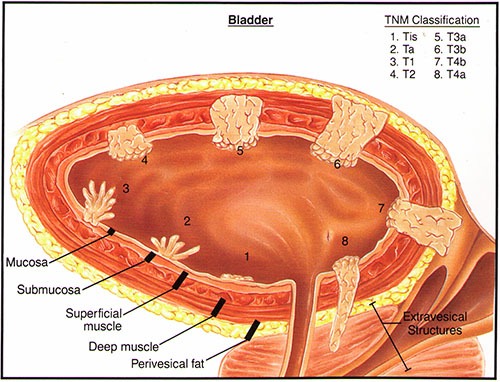
Cancers that are confined to the mucosal layers are termed non-muscle invasive or superficial bladder cancers.
Invasive bladder cancers are those that penetrate into the muscular layer of the bladder wall and require more aggressive therapy.
Bladder cancer symptoms
Bladder cancer symptoms are usually diagnosed after one of the below become apparent:
- Blood in the urine visible to the naked eye (macroscopic haematuria)
- Blood in the urine detected microscopically
- Painful urination, called dysuria, in the absence of infection (a symptom of carcinoma in situ)
All three of these bladder cancer symptoms are common and have many benign causes, but warrant complete and appropriate investigation to rule out urinary tract malignancy.
Diagnosis of bladder cancer
Initially, to bladder cancer diagnosis comprises of an analysis of a urine sample should be undertaken by voided urinary cytology or VUC, which involves collecting a urine specimen and examining it under the microscope for cancer cells.
Urine culture might also be undertaken to exclude urinary tract infection, especially if dysuria is present in the absence of blood in the urine.
In cases of painless macroscopic haematuria, bleeding from the urinary tract above the bladder must be excluded, usually by a CT scan. Specifically, it is important to rule out cancer of the kidneys. The lower urinary tract is then investigated using cystourethroscopy, a procedure which involves the insertion of a small tube with a camera on the end into the bladder under local or general anaesthesia.
Urinary cytology is usually negative when superficial bladder cancers are diagnosed; it is important to have a cystourethroscopy regardless of your cytology results.
Bladder cancer treatment options
Bladder cancer treatment will vary depending on the stage of the cancer and some of the other considerations below.
Superficial bladder cancer treatment
Superficial bladder cancers account for the majority of diagnoses. These tumours are confined to the bladder mucosa and are treated in the first instance by endoscopic resection. Samples of the bladder muscle will also be undertaken to ensure that muscle invasion has not occurred.
Additional treatment by intravesical chemotherapy may also be recommended if you have:
- Multiple tumours
- A high grade tumour(/s)
- A rapidly recurring tumour(/s)
Intravesical chemotherapy or immunotherapy involves the introduction of a drug directly into the bladder in an attempt to prevent a recurrence. The most commonly used agent is called BCG, this drug is administered once a week for six weeks. Following initial treatment, a three-year maintenance program of BCG in three weekly installations every six months is now generally recommended for most superficial bladder cancers.
As superficial bladder cancers tend to recur over time, regular check-ups are necessary lifelong. This is called a bladder cancer surveillance program. It will involve periodic repeating of urinary cytology and cystourethroscopy. The interval between check-ups depends on several factors: how many tumours are present in your bladder, the grade of the tumours and how frequently the tumours recur.
It is important to comply with your surveillance program as approximately 15% of superficial bladder tumours progress to invasive cancers.
Carcinoma in situ treatment
This is a pre-invasive form of bladder cancer which is confined to the bladder mucosa at diagnosis. These tumours are aggressively pre-malignant.
Symptoms include irritative lower urinary tract symptoms, such as dysuria in the absence of infection. Because the symptoms mimic urinary tract infection, patients may be inappropriately treated with empirical antibiotics.
Voided urinary cytology is generally positive and cystourethroscopy is mandatory where carcinoma in situ is suspected. Areas of carcinoma in situ are visible to the naked eye and appear as reddened, raised patches in the bladder wall. Where possible, these are treated with local ablation and generally also require BCG therapy.
Again, regular check-ups are necessary lifelong.
Muscle-invasive bladder cancer treatment
Muscle invasive bladder cancer may occur spontaneously or from areas of superficial bladder cancer or carcinoma-in-situ. Muscle invasive disease is an aggressive form of bladder cancer requiring early intervention and carefully follow up. Complete removal of the bladder, called a radical cystectomy, has the potential of cure and is usually recommended. Treatment with radical pelvic radiotherapy may also be an option.
In suitable patients, functional re-construction known as the neo-bladder formation is possible and desirable. This surgically constructed neo-bladder is created out of a section of bowel which is completely resected and refashioned into a pouch that replaces your cancerous bladder. The ureters and the urethra are surgically attached to this neo-bladder. The bowel ends are rejoined so your bowel functions as normal.
Bladder cancer frequently asked questions:
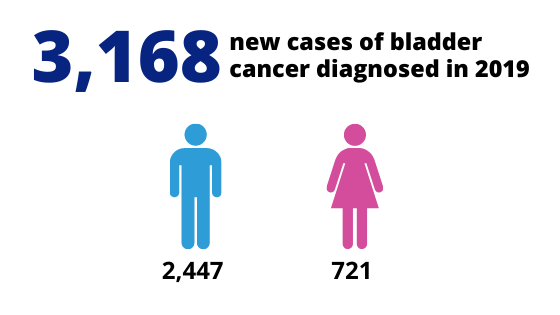
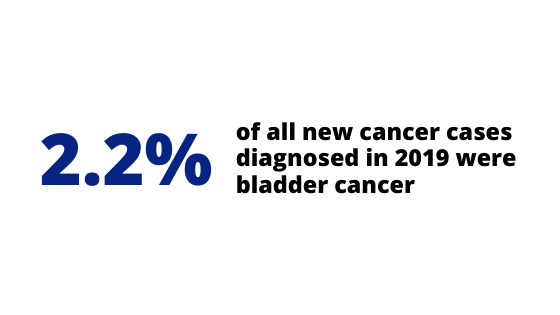
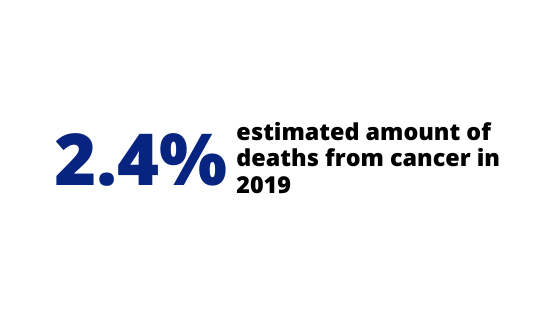
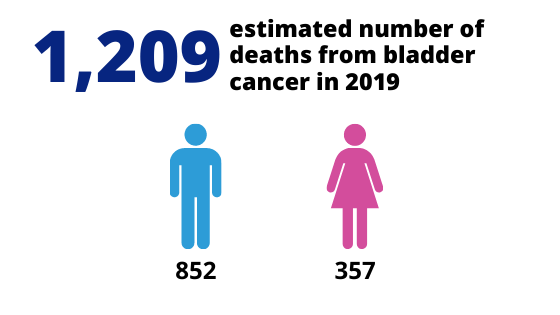
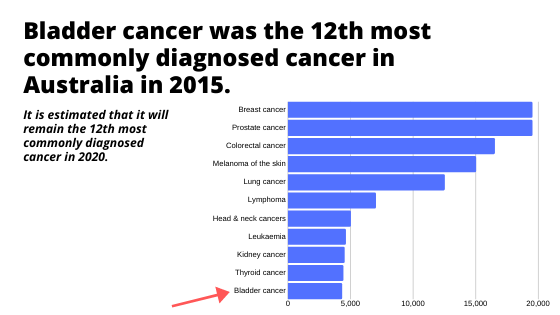
Bladder cancer statistics
The below statistics are referenced from The Australian Institute of Health & Welfare
Dates data collected March 2019